What Everyone Should Know About the Flu Vaccine

It’s that time of year: pumpkin spice, fall festivals, and gorgeous foliage. But throughout this season of autumnal joy lurks the start of the ever-menacing influenza virus season and subsequent “viral” (pun intended) campaign about the necessity of the influenza vaccine. ‘Tis the flu vaccine argument season, so grab your salted caramel latte, pumpkin scone, and a cozy sweater: let the debates begin! These debates have become particularly virulent (okay, last pun) thanks to social media and irreverent physicians like ZDoggMD. The word “vaccine” seems to be a “trigger” now and this is apparent at any dinner party, school board meeting, or social media post. The topic has become so polarized it’s borderline religious—you either believe in flu vaccines or you don’t. Forget the scientific inquiry!

The flu can be deadly
I worked for several years as a pediatric nurse practitioner in the critical care setting (intensive care for very sick children). I have seen what the influenza virus can do to a child. I’ve been the one giving chest compressions to a seven year-old girl when her cardiovascular system collapsed due to shock from the flu virus. I have never been so tired and anxious as I was during the H1N1 flu pandemic of 2009. If the emergency department called saying they needed a bed in the ICU for a child with H1N1, I knew it was going to be a busy and exhausting shift. These kids got sick quickly and were at death’s door faster than any other infectious disease process I had seen in my career. This lasted for weeks and weeks; while at work, I was in a constant state of fight-or-flight. But I was fortunate—I was not sick and these children were not my own, though I loved and cared for them. I longed for an end to the suffering.
I have a very reasonable respect for the influenza virus, especially when it comes to children. Between the years of 2010 and 2016, the virus caused 675 pediatric deaths with approximately one third of those being children under the age of two years. The majority of these children died within ONE WEEK of symptom onset, many of them before they even reached the hospital! Half of the children who succumbed to flu-related death were not “at risk,” meaning, they had no significant medical comorbidities that would render them more susceptible to severe complications than the average child. Among the children who died, the vaccination status of 477 was known; 22% were fully vaccinated for the flu, yet died anyway, demonstrating that the influenza vaccine is not absolute protection. Children who had no known medical condition were less likely to have received the influenza vaccine; less likely to have gone to the hospital; and less likely to have received antiviral treatment. This demonstrates a lack of general public awareness of how devastating the flu can be and how quickly it can claim a young life.
Is flu vaccination safe and effective?
So to “flu shot” or not to “flu shot”? That is the question! For those readers shaking their heads at the ridiculousness as to why this is even a question; I implore you to consider why some people will be reluctant. But first things first: there are a few facts and terms that need to be understood for the sake of argument. The influenza virus, also known as “the flu”, has main types (i.e. A,B,C) and many sub-types (i.e. H1N1, H3N2 etc). There are a multitude of other respiratory illness that mimic the flu and are identified by the Center for Disease Control (CDC) as “influenza-like illnesses” or ILI. So, if you are researching reputable resources, take note of the wording. Two thirds of people who reportedly have “the flu” actually have influenza-like illness. The CDC and US policy makers have been criticized for inflating the number of actual influenza illnesses and death because ILI as well as pneumonia are lumped into one number of influenza infections and deaths. The “flu shot” or the influenza vaccine is supposed to contain the types/subtypes of the influenza viruses that are most likely to circulate within communities each year. Just because one receives a flu vaccine does not mean he or she is immune to other influenza subtypes or certainly all influenza-like illnesses. This year, the inhaled vaccine, which was previously considered completely ineffective, is back, so there are two options: the injected or inhaled vaccine.
The injected vaccine comes in different options: trivalent (three strains of flu) and quadrivalent (four strains of flu). There are a few different manufacturers of each type and different age restrictions for each. Some contain thimerosal, a mercury preservative; which, can be dangerous. According to the FDA: “depending on the vaccine formulations used and the weight of the infant, some infants could have been exposed to cumulative levels of mercury during the first six months of life that exceeded Environmental Protection Agency (EPA) recommended guidelines for safe intake of methylmercury.” There is a newer one available for those with egg allergies, but only approved for those over 18 years of age. The inhaled vaccine is a live virus vaccine and is contraindicated in some conditions; such as, pregnancy, children less than two years old, adults over 50, young children with asthma and wheezing, immunosuppressed people and their caregivers, underlying serious medical conditions, and previous Guillain-Barre after influenza vaccine.
So, are they “safe and effective”? An obvious place to look for research on the influenza vaccine would be the Cochrane Collaboration database. This is where unbiased, non-governmental scientists (detached from pharmaceutical company influence or policy-making) review the large body of research on various topics. The main result of the Cochrane review on the influenza vaccine in adults is this:
“Influenza vaccines have a modest effect in reducing influenza symptoms and working days lost. There is no evidence that they affect complications, such as pneumonia, or transmission.”
“Vaccines increase the risk of a number of adverse events, including a small increase in fever, but rates of nausea and vomiting are uncertain. The protective effect of vaccination in pregnant women and newborns is also very modest.”
For healthy adults 18-65 years of age, depending on the year, the influenza vaccine is usually about 30-50% effective. When it comes to the pediatric population, the Cochrane database is quite critical of the body of “evidence” used by physicians and public health policy makers. While they found that the vaccine is effective in preventing the flu in children older than two, there was little evidence available for children under two—this demographic being most affected by severe illness and death from the disease. Only one study of safety and/or efficacy for children under two was identified, yet it is the current recommendation to start giving it yearly starting at 6 months of age. One study we found demonstrated the lack of efficacy of the influenza A vaccine in the prevention of illness in children under the age of two (in Japan). A literature review also found that the influenza vaccines were associated with serious harms, albeit rarely. The authors even include this troublesome finding: “The review showed that reliable evidence on influenza vaccines is thin but there is evidence of widespread manipulation of conclusions and spurious notoriety of the studies.”
According to the most recent report from the Advisory Commision on Childhood Vaccines, 275 of the 332 adjudicated settlement cases for vaccine injury and death over just a nine month period (2017) were for the flu vaccine, mostly serious injury, but four deaths were attributed to the vaccine also, making one of the riskiest vaccines on the market (Department of Justice Report, September 8, 2017, Sarah Duncan, Trial Attorney). The following conditions are listed in the adverse reactions that received government compensation: encephalitis, Guillain-Barre Syndrome, transverse myelitis, demyelinating injury, chronic inflammatory demyelinating neuropathy, Stevens Johnson Syndrome, fibromyalgia, acute disseminated encephalomyelitis, myoclonic seizures, acute renal failure. There are 16,777 VAERS (Vaccine Adverse Events Reporting System) reports listing serious adverse effects across all types of flu vaccines, including 1336 reported deaths. Keep in mind, these VAERS reports are not proven cases, but rather, reported adverse events that have yet to be investigated; despite this, it is still a concerning number. There are a number of other studies that lend credence to flu vaccine skepticism:
Recent study findings suggest that receiving the injected influenza vaccine increases the risk of other non-influenza respiratory illnesses.
Another study found people who were vaccinated 3 years in a row appeared to have a higher risk of being infected with the dominant flu strain in the latter year, casting doubt on the safety of serial, yearly influenza vaccination for healthy individuals.
Another study had similar findings: repeated vaccination seem to decrease the effectiveness of the vaccine in individuals in subsequent years. The influenza A vaccine was found to be 65 % effective in people not previously vaccinated; effectiveness dropped to 24% in those frequently vaccinated.
A nested case-controlled study found that the trivalent influenza vaccine failed to provide protection against hospitalization in pediatric subjects. This was most especially in children with asthma, who were found to have three times the risk of hospitalization as compared with asthmatic children who did not receive the vaccine.
And pregnant women who received the pH1N1 vaccine in the previous season were found to be at increased risk of miscarriage in the 28 days following immunization.
While more studies should be conducted to verify these results, this ever-growing body of scientific studies and literature reviews suggest that concerns expressed over the safety and efficacy of the influenza vaccine are not unfounded. Of note, the CDC and AAP (American Academy of Pediatrics) have lists of studies to support their current recommendations. When I researched this topic, a quote mentioned in the writings of Mark Twain came to mind: “There are three kinds of lies: lies, damned lies, and statistics.” Statistics can be manipulated.
So, for some, the risk of the influenza vaccine is not worrisome compared to the perceived benefit, yet to others, the risks of adverse events or unintended consequences documented from the vaccine are enough of a concern to forgo perceived benefits. It is reasonable to say that its effectiveness is suboptimal and that scientific literature on some populations is scarce enough to warrant it unmeritorious of the title of “safe and effective.”
Influenza vaccine is recommended for anyone over six months of age who does not have any conditions to warrant contraindication; however, one should note that as a parent, you have the ultimate say in your child’s health. Physicians and nurses who will not have a reasonable and honest conversation about the safety and efficacy of this vaccine lack professionalism. They are not allowing you “informed consent” when they gloss over the risks and over-exaggerate the benefits. The influenza virus is usually a self-limiting illness for the majority of children and adults. Complications are usually the result of bacterial co-infection and sepsis.
You herd wrong
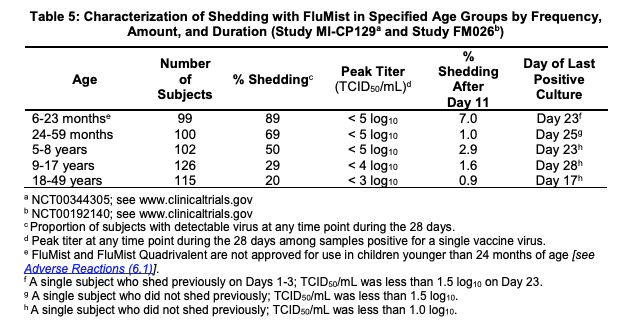
Some might argue the altruism of people who receive and give the influenza vaccine to their children to protect others. Know that children who receive the inhaled vaccine were found to shed the virus for up to 28 days:
Furthermore, the Lancet found that many people infected with influenza have no symptoms. This is important information to consider when asymptomatic carriers, vaccinated or unvaccinated, could be an important source of transmission within communities. Even those fully vaccinated who might have less severe symptoms are not compelled to stay home from work or school because they are just not that sick. These individuals can still spread the infection to vulnerable children and adults. If you have fever or feel sick, it is prudent to avoid the holiday party where your cousin’s toddler or elderly granny will be. Flu shots do not give the green light to carry on as usual.
How to avoid the flu without the flu vaccine
Here are a few suggestions on how to avoid and treat the influenza, regardless of one’s vaccination status:
Nutrition: A well-nourished body is one that can fight off illness. In addition to multivitamins, incorporate immune-boosting nutritional supplements for the entirety of the flu season. This should include vitamin A, vitamin C, vitamin D3, and probiotics. A low-sugar, whole-foods, diet is recommended.
Hydration: Fluids are essential for the lymphatic system to prevent and fight off infections. Try water with lemon as opposed to sugary drinks.
Prevention: Wash your hands often; isolate your family from avoidable public places; try elderberry syrup which has promising symptom management of influenza and influenza-like illnesses, but note that pediatric information is lacking.
If you or your child comes down with the flu and you want to limit the suffering with an antiviral, make sure to see your doctor and get Tamiflu as soon after the onset of symptoms as you can.